What is Diabetes?
Diabetes mellitus(DM) is a metabolic disease involving elevated blood glucose levels. The term diabetes mellitus originated around 250-300 BC. Diabetes is one of the most common chronic diseases in the country and worldwide, despite having an effective medical system at present. Diabetes mellitus can affect people of any age, from children to the elderly. There are different types of diabetes, and there are various treatments for it.
A.Primary Diabetes:
There are three main types of diabetes: type 1, type 2, and gestational diabetes (diabetes while pregnant).
Diabetes Type 1
If you have type 1 diabetes, you’ll need to take insulin every day to survive. Type 1 diabetes is caused by an autoimmune reaction (the body attacks itself by mistake). Around 5-10% of the people who have diabetes have type one diabetes. Currently, no one knows how to prevent type 1 diabetes.
Diabetes Type 2
With type 2 diabetes, your body doesn’t use insulin well and can’t keep blood sugar at normal levels. Type 2 diabetes can be prevented or delayed with healthy lifestyle changes. 90-95% of people with diabetes have type 2, according to the American Diabetes Association.
Gestational Diabetes
If you have gestational diabetes, your baby could be at a higher risk for health problems. Gestational diabetes develops in pregnant women who have never had diabetes. Your baby is more likely to have obesity as a child or teen and has a higher chance of developing type 2 diabetes later in life.
Comparison of two types of diabetes mellitus:
| Traits | Insulin-dependent diabetes mellitus(IDDM) | Non-insulin-dependendent diabetes mellitus(NIDDM) | |
| 1. | Synonym | Type 1, Juvenile-onset diabetes | Type 11, adult-onset diabetes |
| 2. | Age of onset | Usually during childhood or puberty.(<20yrs) | Frequently after age 35. (>yrs) |
| 3. | Nutritional status at the time of onset of disease | Frequently undernourished | Obesity usually present |
| 4. | Prevalence | 10%-20% of diagnosed diabetics | 80%-90% of diagnosed diabetics |
| 5. | Genetic predisposition | Moderate | Very strong |
| 6. | Defect or deficiency | Beta cells destroyed | The inability of beta cells |
| 7. | Ketosis | Common | Rare |
| 8. | Plasma insulin | Low to absent | Normal to high initially |
| 9. | Acute complications | Ketoacidosis | Hyperosmolar coma |
| 10. | Oral hypoglycemia drugs | Unresponsive | Responsive |
| 11. | Treatment with insulin | Always necessary | Usually not required |
Clinical features:
A.Common: • Thirsty, Dry mouth • Polyuria • Polydipsia(increased thirst)• Polyphagia(increased appetite) • Fatigue • Tachycardia • Nausea • Headache • Weakness • Loss of weight
B.Others: • Dehydration • Hypotension• Hypothermia • Confusion • Drowsiness • Hyperventilation
• Muscle wasting
Investigation of Diabetes mellitus:
1. Urine Examination: • Suger • Ketone bodies
2. blood glucose determination:
A. Healthy people:
I. Fasting plasma glucose levels:3.6-5.5mmol/l
II. .2hrs after food, random or 75gm glucose:<7.8mmol/l
B.In Diabetes mellitus:
I. Fasting plasma Glucose :>7.8mmol/l
II. 2hrs after food, random or 75gm glucose :>11.1mmol/l
C. Impaired glucose tolerance:
I. Fasting glucose:5.5-7.8mmol/l
II. 2hrs after food, random or 75gm glucose:7.8-11.1mmol/l
3. Oral glucose tolerance test(OGTT)
4. Glycosylated HbA1 test:
Normal: 4.2-6.4of total Hb
It increases in poorly controlled diabetes mellitus and maybe more than 9%
—–
4. Other investigation:
I. Urine for proteins
II. A full Blood count(CBC)
III. Blood urea
IV. Blood electrolytes
V. Blood lipid profile
Management of DM:
1. Diet: It helps a lot in controlling sugar if patients follow their diet
Low-fat dairy, fresh food, fruits, high protein & fibre-rich diet.
Always avoid high-sugar food such as sweetened sodas and High Suger desserts.
Don’t drink an excessive amount of alcohol.
2. Exercise: Regular exercise (more than 150 minutes per week), such as walking, aerobics, swimming, cycling
3. Insulin: Since T1DM is primarily a disease caused by the absence of insulin, the mainstay of insulin administration or insulin pump treatment is daily injections.
Two types of insulin preparation are commercially available-
-Short-acting insulin(Soluble insulin)
-Long-acting insulin(insoluble insulin)
4. Drug:
Oral hypoglycaemia drugs. e.g., Sulfonylurea-Autohexamide, Tolbutamide, Glibenclamide.
Specific subclasses include Biguanides (Metformin), Sulfonylureas, Alpha-Glucosidase Inhibitors, Thiazolidinides, Glucagonlik-Peptide-1 Agonist, Diptipil (Peptidev)) inhibitor. Metformin is the first line of prescribed diabetic drugs and lowers basal and postoperative plasma glucose.
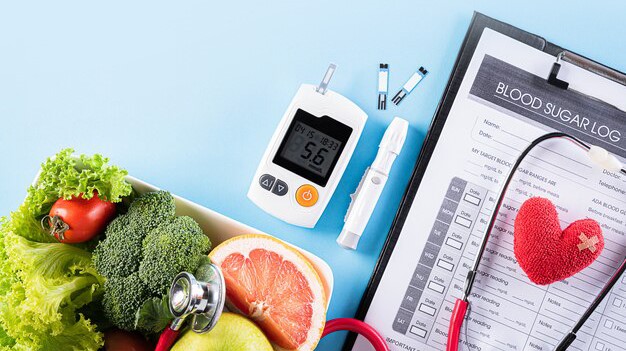
Self-monitoring:
The patient can monitor glucose independently by using a blood glucose meter for effective diabetics management, such as helping to regulate meal schedule medicine taken, including insulin.
Complication:
Blindness: Long-term complications of diabetes include retinopathy with a potential loss of vision.DM is also a common cause of blindness in adults aged 20 to 74 years in the United States. Diabetic retinopathy contributes to 12000 to 24000 new cases of blindness annually, and treatments generally consist of laser surgery and glucose control
Nephropathy leading to renal failure: Renal disease is another significant cause of morbidity and mortality in DM patients.
Peripheral neuropathy with risk of foot ulcers, amputations, and Charcot’s joints; and autonomic neuropathy causing gastrointestinal, genitourinary, and cardiovascular symptoms and sexual dysfunction.
Diabetes ketoacidosis: The most acute complication of DM is diabetic ketoacidosis (DKA), which typically presents in Type1DM. This condition is usually due to inadequate dosing, missed doses, or ongoing infection.
Diabetic retinopathy: The duration of diabetes is the most crucial risk factor for developing diabetic retinopathy.
Gestational Diabetes are at a higher risk for cesarean delivery and chronic hypertension.
Pregnant patients with Type2DM generally have a better prognosis of neonatal and pregnancy complications than those with Type1DM. Generally, neonates of DM mothers will present with hypoglycemia and macrosomia.
Conclusion:
Diabetes can be controlled effectively by providing adequate medical care to diabetic patients and implementing appropriate lifestyle changes. Additionally, nurses and pharmacists should receive extensive training in order to assist diabetic patients in learning about their condition on an individual basis.
Please note: I have needed three pictures for this article.
- Pancrease picture from the net
- Glucometer testing time by DM PT.(prepare by iqbal apon & me)
- Healthy Food dishes for DM PT.(prepare by me & iqbal)